A 45 year old male with bilateral pedal edema
This is an E logbook to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent. Here, we discuss our individual patient's problems through series of inputs from an available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence-based inputs. This E-logbook also reflects my patient-centered online portfolio and your valuable inputs in the comments are welcome.
I have been given this case to solve in an attempt to understand the topic of " Patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations, and come up with a diagnosis and treatment plan.
CASE PRESENTATION:
This is a case of a 45 year old male, gas welder and tractor driver by occupation who presented with chief complaints of :
- Swelling of both lower limbs since 4 days
HISTORY OF PRESENTING ILLNESS:
Patient was apparently asymptotic 5 years ago then he developed grade-I shortness of breath which was insidious in onset and gradually progressed to grade IV 6 months back.
He has bilateral pedal edema since 4 days which is pitting type insidious in onset , aggravated on standing for long hours, relieved on taking rest. It was associated with severe knee pains since 6 months.
He has been experiencing pedal edema on and off since 1 & 1/2 years.
PAST HISTORY:
K/C/O : Diabetes mellitus since 6 yrs
Hypertension since 6 months
Epilepsy since 1and 1/2 years
Not a known case of tuberculosis,asthma
TREATMENT HISTORY :
FAMILY HISTORY: insignificant
PERSONAL HISTORY:
Diet : Mixed
Appetite:normal
Sleep : Inadequate
Bowel and bladder: regular
Addictions:
Alcohol consumption since 20 years (1whisky bottle per day for 4 days in a week)
Occasional toddy consumption
Zarda pan chewing since 6 months
GENERAL EXAMINATION:
Patient was examined in a well lit room, after taking informed consent.
He was conscious,coherent and cooperative and well oriented to time place and person
Pallor: present
No Icterus
No Cyanosis:
No Clubbing of fingers
No koilonychia
No Lymphadenopathy
Pedal edema present


VITALS:
Temperature : Afebrile
Pulse Rate: 75bpm
BP:
RR: 18 cpm
SYSTEMIC EXAMINATION:
CVS: S1 and S2 heard. No murmurs
RS : NVBS +, BAE +
Per abdomen: soft , non tender
CNS: HMF intact
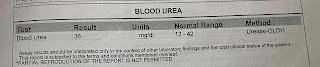
INVESTIGATIONS:
On 18/10/2021
CUE: albumin:+ 4
Sugar: +
Pus cells:5-6
Epithelial cells:3-4
Red blood cells:nil
Crystals and casts:nil




On 30/10/21:
Serum creatinine:2.6mg/dl
Potassium-4.6 mmol/L
Reticulocyte count:0.6
Hemogram:
Hb : 8.7 gm/dl
TLC : 9600
Neutrophils: 53 %
Lymphocytes: 38%
PCV: 24.3
Platelets: 3.15
LFT:
Total bilirubin:0.32
Direct bilirubin:0.13
ALT:12
AST:15
AKP:336
Total protein:4.5
A/G:0.97
Serology: negative
ECG:

USG ABDOMEN:

TREATMENT:
- Tab. Ecosprin-AV/OD/HS
- Tab. Livogen/PO/OD
- Tab NODOSIS 500mg/PO/BD
- Tab PAN 40 mg PO/OD
- Fluid restriction <2liters/day
- Tab. CEGLIM -1 PO



Comments
Post a Comment